OFFICE HOURS |
OFFICE INFORMATION |
||
|
Monday - Friday |
8:30am - 4:30pm |
980 Westfall Road |
[Phone] 585.442.1110 |
 |
I Would Like To:
|


LASER endoscopic myotomy
(minimally-invasive endoscopic swallowing pouch LASER surgery)
The esophagus (swallowing tube) has two muscular sphincters which regulate the passage of food into the stomach. The upper esophageal sphincter is located in the neck, about three inches below the "Adam's apple." It is a semi-circular muscle called the cricopharyngeus. Normally, it relaxes with each swallow to allow the food to pass. When it does not relax with swallowing it is considered a dysfunction, and may produce the following symptoms:
1. sense of food getting stuck low in the neck
2. a 'lump' in the throat
3. difficulty swallowing, especially solids
Cricopharyngeal dysfunction can continue for years without the symptoms getting worse, however, most people affected find that it is progressive.
A "Zenker's" is the most common type of an abnormal pouch that forms in the upper esophagus, primarily caused by long-standing cricopharyngeal dysfunction. It is a blind sac (= diverticulum) that is symptomatic because undigested food collects there, and when severe, is regurgitated.
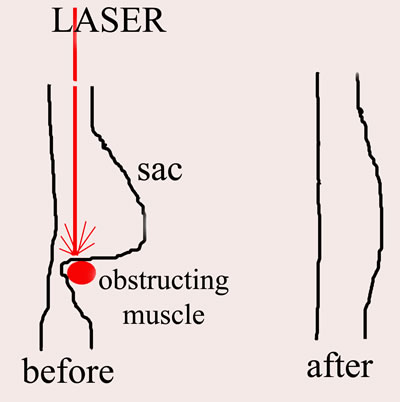
Most x-ray swallow-studies show a narrowing of the esophagus in the neck (see figure below) with or without the blind sac collecting x-ray contrast (in white).
Cricopharyngeal dysfunction with or without a Zenker's diverticulum occurs because the cricopharyngeus muscle does not work properly (by not relaxing when one swallows), therefore all therapeutic options must address this muscle.
⇒ Observation. Although the difficulty swallowing is considered progressive by most, treatment is not absolutely mandatory.
⇒ BoTox injections. Botulinum toxin temporarily paralyzes any muscle it is injected into, including the cricopharyngeus. This is a temporary solution (2-4 months, on average), for those who are symptomatic but can not or wish not to have a more definitive procedure attempted. One advantage is that it is performed under local anesthesia in our clinic.
⇒ Open cervical cricopharyngeal myotomy with or with diverticulum (open cervical = neck incision; cricopharyngeal myotomy = cutting the cricopharyngeus muscle; diverticulectomy = removal of pouch). This was the standard of care until recently. The major disadvantages include a 7-day hospitalization with a feeding tube, risk of temporary or permanent paralysis to the left vocal cord, and a 10% rate of recurrence.
⇒ LASER endoscopic cricopharyngeal myotomy (LASER endoscopic = through-the-mouth with a LASER beam). The procedure is the latest standard of treatment, when it can technically be done. Interestingly, those with the Zenker's (pouch) generally do not need to have it removed (see figure below). The myotomy is sufficient in most cases to solve the problem. The procedure is considered MINIMALLY-INVASIVE.
Unique benefits of LASER procedure: this minimally-invasive procedure allows quicker healing, with only a 1-2 day hospitalization for most patients. You typically begin eating the morning after surgery, and there is no incision in the neck.
The downside: 10-15% of patients will have anatomy that would make it technically impossible to do the LASER procedure. Those patients would then require the open cervical procedure, or another option. The 10-15% can NOT be identified prior to surgery. All patients are asked in advance which would be their second-choice treatment if the LASER procedure can not be done.
 |
Pictures & Videos

Pre-operative endoscopic view of the throat in a patient
who has a symptomatic Zenker's pouch. Note all of the
frothy secretions that seem to be pooling in the throat.

Post-operative endoscopic view of the same patient a few
weeks after having an LASER myotomy. Note the abscence
of secretions pooling in the throat.
Video recording intra-operatively of a LASER crico-pharyngeal myotomy in a patient with a moderate sized
Zenker's diverticulum. The view through the operating
microscope is the same that Dr. Haben would have while operating. The procedure is done with a "green light"
532-nm KTP LASER that is delivered through a glass fiber
cable. The entire procedure is completed through the mouth
without incisions in the neck skin (= minimally invasive).
A metal scope is placed into the mouth to hold open the
throat during the surgery. The final incision in the muscle is
approximately 1 inch.
Post Operative Instructions
Once discharged from the hospital, there are no dietary restrictions. On the contrary, you are encouraged to "test" your swallowing against a wide variety of food consistencies, especially those which gave you difficulty pre-operatively. Begin slowly, however you should be consuming a normal diet by the end of the first week.
Work and activity: people respond to general anesthesia differently. Some only feel 'groggy' for a few days following surgery, while others are 'out-of-it' for 7-10 days. Your body and common sense will dictate when you can resume physical activity/work. Typically, 1-2 weeks recovery will suffice.
Medications: most will be given a prescription antibiotic to take each morning for one week. Pain medication will also be provided, however, most only need extra-strength tylenol or ibprofen. If you are experiencing severe discomfort or pain that is increasing day after day, you should call us immediately.